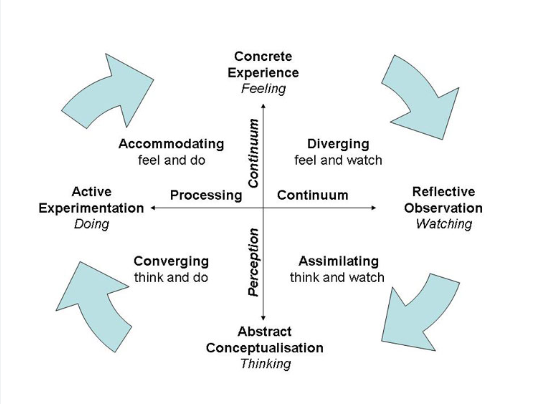
The assignment brief of 'taking ownership of one's own learning' was a new concept for me. Through all these years of education, I always assumed learning to be a mere transfer of knowledge from one source to another. In my case, the source has mostly been an educator, reference material, or peers. For a long time, learning was a one-way street for me where only the delivery from the source was focused on while my perception of that knowledge went completely unnoticed. As a result, metacognition of the whole learning process was never thought of and I failed to understand and reflect adequately on it. Nonetheless, through this failed attempt I reflected on a source of knowledge that I have been following for years but did not realise its potential until now. This source of knowledge was learning from my experiences. Jan De Houwer et al. 2013 defines learning as changes in behaviour learned from past experiences. I realised that only after I went through the examples of my batchmates on the discussion board using Kolb's experiential learning theory to reflect on their life experiences, I realised I have had a similar learning cycle. I first heard about the Kolb's experiential theory in one of the lectures of this module. At that instance, it came across only as a piece of information but now having had a concrete experience of failure I could relate to the theory on an analytical level. I could understand the stages of the theory and correlate it with my personal experiences. The first attempt was the concrete experience I needed next step was reflective observation. Trying to reflect on the experience was a mixed bag of emotions I was equally nervous and confused, it was a hazy cloud even after doing my SWOT analysis.
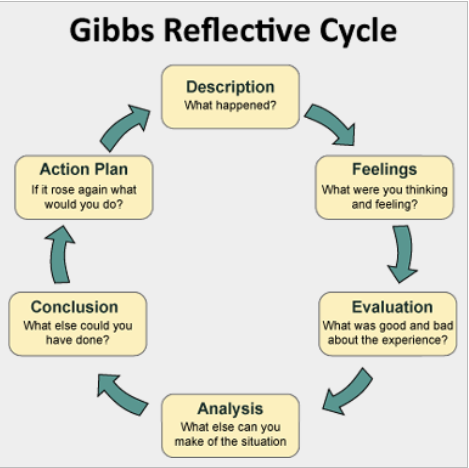
After a couple of failures I relied on Gibb's reflective cycle for my reflective journey . It has six stages to reflect on an event and it also asks the reflector questions to address every stage. I realised during the module workshops that answering questions to reflect or as feedback is easier for me than directly giving a summary of an event, this makes sure I have bullet point information and I do not miss anything important. The first stage of the cycle is the description of an event, writing an assignment on 'who is an advanced physiotherapy practitioner', and knowing the necessities to become one was my end goal. The next stage is feeling, I remember feeling underconfident about both passing the assignment and reaching my end goal this was because of the confusion and unclear learning needs. I was lost learning too many unrelated things on the surface without reaching into the depths of a particular topic. I also failed in choosing the right learning activities and they were not powerful enough to give me clarity about the topic I was learning.
The next stage of Gibb's reflective cycle was evaluation, reading my assignment was not helping me understand my mistakes until I gave close attention to the evaluator's feedback and took constructive criticism from my peers. It opened a two-way street of knowledge for me where I could understand and ask what did not go well for me. I certainly felt at ease understanding my mistakes but also knowing there was a scope for improvement. The cluster in my mind started to unwind and I could start picking up threads of one thing at a time, determined to not repeat those mistakes. During this process, I understood that my major focus was on the topic rather than the learning of the topic itself. It was at the stage of analysis where my reflection took a new turn, while I understood my mistakes in structuring the assignment, I also understood a few gaps in my topic itself.
While, the aim of becoming an advanced physiotherapy practitioner (APP) began as a well sought after professional position, I did not know what are the duties of an APP. I learned that the responsibilities of an APP are far more than the clinical scope of a professional physiotherapist. According to the Chartered Society of Physiotherapy, advanced physiotherapy practice involves an inclusive and holistic approach to the profession which includes four pillars of research, education, service development, and professional leadership (Advanced practice in physiotherapy Understanding the contribution of advanced practice in physiotherapy to transforming lives, maximising independence and empowering populations ). I remember being left with the feeling of 'do I truly want to become an APP?' while writing the assignment, I was not fully committed to my end goal! I could conclude that the responsibilities and the job role demand for becoming an APP were pressurising me more than inspiring me. As a result, I could not build appropriate sub-learning needs along the main topic and failed to convince myself as an aspiring learner.
Despite uncertainties around the job title and role, my interest in musculoskeletal (MSK) physiotherapy has been paramount since my undergraduate years. I learned about the role of a musculoskeletal physiotherapist as a first contact practitioner (FCP) while researching for the assignment and that interested me. FCPs are clinicians with MSK experience and advanced clinical practice skills to assess, diagnose and manage all MSK conditions including complicated cases (Goodwin et al. 2021). This gave rise to my abstract conceptualisation from Kolb's learning theory that I may or may not want to take the added responsibilities of becoming an APP in the future but what I can do currently is develop my expertise to become an advanced musculoskeletal physiotherapist. The last stage of Gibb's reflective cycle was to make an action plan. Hence, with an aspiration to enhance my learning and improve my practice using a self-directed Continued Professional Development (CPD) approach, I decided to use this opportunity of writing this assignment to learn a topic which I do not feel very confident about from a perspective of an advanced musculoskeletal physiotherapist.
The shoulder has always been a subject of my interest, throughout my undergraduate course and rotational internship I have seen several shoulder cases but most of them have been frozen shoulders, post-fracture rehabilitation, or impingement. Shoulder instability was a topic unintentionally ignored by me, the primary reason being lack of patient exposure. While reflecting on this I also realised I had a certain apprehension about assessing and diagnosing patients with shoulder cases as they were always in tremendous pain which would put me in a position of fear and the other reason was the shoulder special test being too complicated to understand and memorize. To get over these inhibitions and take a step towards advancing my skills in assessing, diagnosing, and managing patients with shoulder dislocation, I prepared a learning contract listing my learning needs.
Anatomy:
Before researching for this assignment, the only information, I had about shoulder instability was in the form of shoulder dislocation related to sports injuries or trauma which were then treated under anaesthesia or surgery and were followed by a long rehabilitation programme. I had seen only a couple of these cases under supervision in either very acute or very late stages of the condition and could never follow up on their prognosis due to the limitation of time during my rotational placement. Before diving into the pathology of the condition it was important for me to brush up on the anatomy of the shoulder for which I first started with an online learning resource website called Physiopedia (Shoulder Instability 2020) which was a one-stop page collected from different articles and reference books and also continued reading research articles.
The shoulder joint, specifically the glenohumeral joint being a ball and socket type of joint has the maximum amount of mobility (Miniato et al. 2022). Besides this, the anatomy of the glenohumeral joint gives it an added advantage over the hip joint which is the only other ball and socket joint in the human body. This advanced mobility is because of the compromised stability as a result of which, shoulder instability and dislocation cases are very common (Abrams and Halleh Akbarnia 2022). Shoulder instability is defined as loss of shoulder comfort and function due to undesirable translation of the humeral head on the glenoid fossa (Nicolozakes et al. 2021). I learned that the dynamic mobility of the shoulder is attributed to the static and dynamic shoulder stabilizers (Shoulder Instability 2020). The static stabilizers included adjacent shoulder ligaments namely the superior glenohumeral ligament which prevented inferior and anterior translation, medial glenohumeral ligament limiting anterior translation while abducting the humerus in the low and mid range and inferior glenohumeral ligament which restrains humeral translation in all directions during 45 degrees abduction and beyond (Baba 2023). The dynamic stabilizers include the surrounding shoulder joint muscles primarily rotator cuff muscles, long head of biceps, and deltoid and secondary muscles including teres major, latissimus dorsi, and pectoralis major (Guerrero et al. 2009). Besides the ligaments, the glenoid labrum also contributes to the static stability of the joint by increasing its depth (Guerrero et al. 2009). The bony composition and of the joint structures like the shallower glenoid fossa and bigger spherical head of the humerus also contribute to increasing the concavity (Dalton and Snyder 1989).
Reading this information through research articles felt like an everyday experience. Even though it required high amounts of concentration to comprehend, anatomy being my area of interest kept me going. What caught my attention was learning from the online resource website. It had important information collected from different websites as a summary posted on a single page. It was a good overview of the entire topic but to dive deeper into the topic, I needed more than just a summary in which case research articles or reference textbooks will continue to be my primary source. Hence, I was doing a constant to and fro between the learning resources and activities.
Types of instability:
After learning about the shoulder anatomy, the next step was the type of instability. Continuing my learning on the website, shoulder instability was classified based on the direction of instability as anterior, posterior, inferior, or multidirectional instability (Brukner & Khan's 2023). The next classification is based on the mechanism of the injury as traumatic and atraumatic (Shoulder Instability 2020) The last type of classification used by clinicians to make the diagnosis of the type of instability and base their treatment on it is Stanmore's triangle classification. When I first read about this through the website, I could not comprehend it very well. There was a diagrammatic representation of the triangle and explanation in words but that was not enough for me to understand the concept.
This was my cue for my next resource of learning which was a YouTube video, what was different in the video than the articles I read was how it set a background story and explained with a patient's movement example. The video clarified that traumatic instability occurs through ligaments or labral tears while atraumatic instability is often asymptomatic and occurs through hyperlaxity, both of them are structural components. The video also introduced me to a new non-structural mechanism of instability called muscle patterning, which is an altered muscle recruitment pattern occurring due to overactivity of superficial muscles and inhibition of deep stabilizers. This causes an imbalance which results in a shearing force and dislocates the glenohumeral joint. The relation between these three types of instability is described best by the Stanmore triangle where a patient may fall under the criteria of less traumatic factor or less muscle patterning factor of instability (Shoulder 2020). The clear storytelling approach of the narrator in the video along with the visual representation in the form of pictures, videos, tables, and x-rays helped me to get to the roots of the cause which was validated by the shift in my confidence level. Watching the video was undoubtedly my prime learning activity for this learning need.
Assessment:
My first source of information was from a reference orthopaedic textbook (Orthopedic Physical Assessment 2021). It provided me with many tests for each type of instability like the anterior release test, anterior drawer test, crank (apprehension) test, fulcrum test, and load and shift test for anterior shoulder instability. For posterior shoulder instability, there are jerk tests, load and shift tests, Norwood tests, posterior apprehension tests, and posterior drawer tests. Feagin test and Sulcus sign for multidirectional instability (Orthopedic Physical Assessment 2021). Learning all this information from the textbook was a challenging experience that required a high amount of concentration and imagination to understand the specific position, grasp, and movement. There were a few images which were depicting these things but were not very clear. My confusion and fear regarding shoulder special tests was only multiplied after this. I was reading through the pages but reaching nowhere. This is when I realised this was not working for me and I needed to move to another source of learning. I relied upon the next best source I knew of watching YouTube videos. They were interesting, easy to understand, and could hold my attention for a longer duration. I could easily understand the patient and therapist's position, and grasp movement intensity and direction. Even though the technique was learned through the videos the confidence to perform these tests was yet to be developed. Pondering upon what to do next I went back to the basics of learning and sought answers in the process. This is when I came across the modified version of Geoff Petty's Learning Cycle Diagram (Petty diagram • Evidence Based Teachers Network 2017). The credibility of this source is questionable but irrespective of that it has provided me a breakthrough in my learning process. This cycle was developed for evidence-based teaching but I used the same steps to support my evidence-based learning. The first step involves checking of evidence and the next step is teaching the evidence to yourself. Learning the special test through reading a reference textbook and then watching videos to help myself learn them completed my first two steps. The next step was performing a task to challenge your learning. Because of the constraint of time and opportunities, I could not practice this on patients at a clinic or through shadowing a supervisor, so I decided to still go ahead and polish my hands-on skills with my peers. I arranged appointments with them to perform the special tests I learned from watching videos.
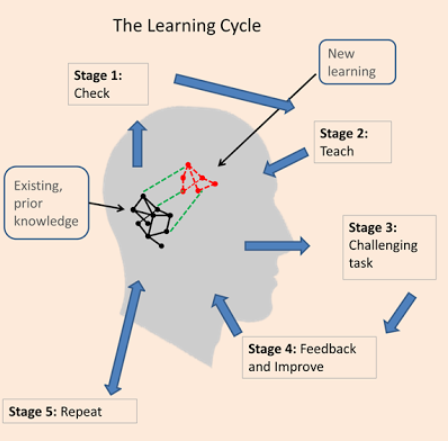
Some of them were from a medical background while others were not. What I was not expecting was to receive such valuable feedback from them which is the next step of the cycle. While most peers from a non-medical background felt comfortable and at ease with the testing. Feedback from a peer of the same profession made a difference, they suggested in the clinical set up I would not be able to perform all these tests together, so you will have to be more prompt at your selection. Another peer reminded me that assessment does not only involve special tests and going back to other basics of assessment like history, observation, and palpation. In the desire to perfect my skill I completely lost track of what is necessary in the practice. I let my fear and apprehension toward shoulder special test drive my learning need in only one direction missing on to other important points. If I would have only blindly followed the unidirectional path of learning and would have not opened pathways to take feedback, I could have never figured out these gaps. Another important thing I realised is the source/ person you are taking your feedback from, if they are not very knowledgeable about the particular topic the quality of your feedback may be compromised. The learning cycle and the resource itself have proved to be very eye-opening for me. The last stage of the learning cycle was to repeat the process that's what I was going to do find new evidence to answer my questions and repeat the process to gain feedback and confidence in my learning.
Management:
Just like for the assessment and diagnosis the management of the shoulder dislocation cases was also a big ball of confusion for me. In most of the acute-stage cases I came across, pain management, strengthening and mobility were the primary goals of treatment. I was somewhat confident in treating the patients in their acute stage but the feeling of stagnation and apprehension would hit as the condition progressed. I used to often wonder will I be able to treat these patients confidently when I go out into the real world.
Going through the already-known resources of reading articles and watching videos gave me the basic idea of which exercises can be administered in the early and the late stages of the condition. A video suggested beginning with closed chain exercises in the early stage to assist the humeral head to sit into the glenoid followed by semi-closed kinetic chain and open chain exercises in the following stages (Physiotutors 2023). All these activities gave me an idea of 'what' to do but were missing the rationale. I needed to know where to start after knowing what kind of instability it is. I was struggling to find a baseline to begin my treatment with.
This is when I moved to my next learning activity of listening to podcasts, this is the one that has interested me the most out of all the learning activities performed for this assignment. I have a habit of listening to podcasts about other non-specific topics but I never used it as a source of my academic or professional learning. When I first started listening to the podcast my only reaction was "Why did I not do it before?" It was like an experience of sitting in a classroom and gathering as much knowledge as I can. The aforementioned point in the podcast was the importance of history to classify the type of instability using Stanmore's triangle and base the treatment on that. Depending on the type, polar type I which involves trauma has to undergo a surgical treatment followed by a rehabilitation. Polar type II which involves atraumatic structural cases, treatment for it should be focused on neurodevelopmental deficit and its related treatment. Polar type III which involves muscular patterning may follow up as per normal rehabilitation. In this case, if no improvement is seen within 6 weeks surgery was suggested rather than waiting for the next dislocation to cause greater damage in young sportsmen by the speaker. In some cases, the pain might turn into allodynia leading to Complex Regional Pain Syndrome which should be assessed and treated accordingly (Matters 2015).
Having said this was one of my favourite learning activities for many reasons; I got to know multi-point of views about a single topic because of having more than one speaker. During the podcast, they also gave a short introduction of their background which created an instant connection and relatability. There was a feeling of comfort knowing there were more people out there struggling with the same topic as me. Although the storytelling approach kept me engrossed there were some instances while listening where I could not grasp certain points because of back-to-back bombarding of the information but I could always go back to listen, another issue was not being able to ask my doubts or questions.
One such question was about the psyche of the patient and its effect on recovery. To find answers to my questions I decided to carry out my one final learning activity of interviewing a supervisor from my internship. They gave me an insight into the biopsychosocial factors affecting the recovery. Patients' belief or experiences throughout the treatment plays an important role in how they perceive the treatment. I remember learning about this concept in one of the lectures in another module. I could now connect the dots and put that theory into my perspective of real-world practice. The supervisor also gave me insights into how physiotherapist's beliefs and practices can affect recovery (Coulthard et al. 2021). The use of manual therapy for the thorax or taping for proprioception varies from the therapist's personal experience and also patient's needs. This interactive session was again very helpful for me as it was learning from the same experiential theory but someone else's experience and perspective. I was a little nervous before asking them the questions but as the conversation progressed, I was comfortable and could grasp and share insights easily.
Implications & Conclusion:
The assignment brief of taking ownership of my learning and then writing a critical commentary on it was a challenging experience for me. This was because of two main reasons, firstly reflection in itself is a challenging practice. It had put me in a place of vulnerability, to accept and understand what did work and did not work for me was not easy. Secondly, thinking about these thoughts of reflection and putting them into appropriate words was another task. Nonetheless, it was made easier with the help of Gibb's reflective cycle, it gave me specific steps to focus on without which I would have been beating around the bush. The process of reflection helped me reach a newer dynamic of learning and even myself as a learner. I would continue to practice it in the future either by use of reflective models or by finding a suitable method like journaling both on the professional and personal front.
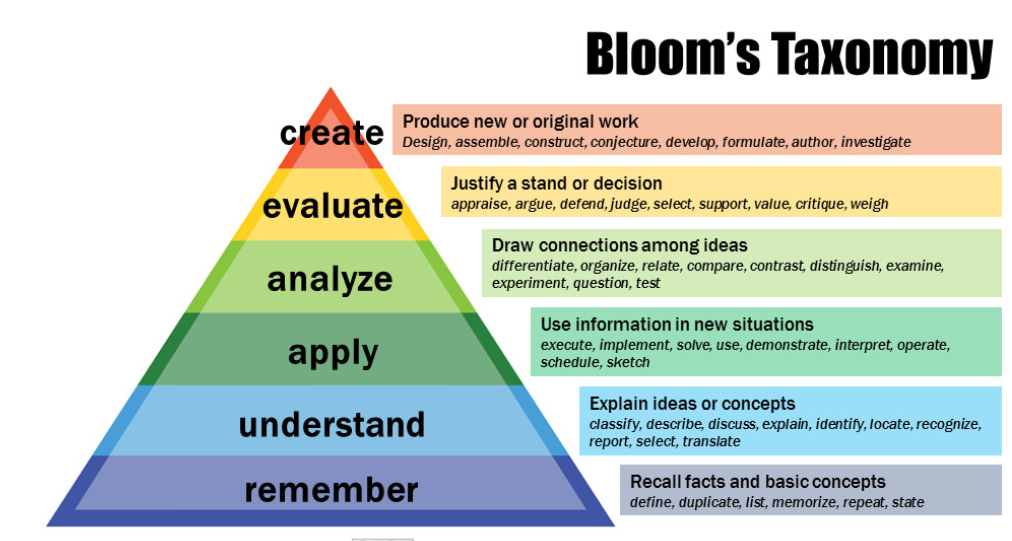
This assignment has helped me get through several barriers in my learning journey which I could have not recognised otherwise. Developing a learning contract and following Kolb's learning theory made me realise that the learning pattern I was following all these years had some loopholes and needed a new outlook. Correlating this entire learning process with Bloom's taxonomy (Appendix 1, Figure 4) helped me get through my biggest barrier of restricted perception of learning. Through the learning activities I had been following before this like reading articles, and textbooks and attending lectures I was only witnessing one or two levels of the taxonomy those being remembering and understanding. Inculcating different types of learning activities like watching videos, listening to podcasts, practicing hands-on skills, peer discussion, and interviewing an expert opened the door for me to explore other components of Bloom's taxonomy. I could not only remember and understand but also apply, analyse, evaluate, and create. Even though, I might enjoy one learning activity more than others I believe all of them were equally important for the process. As for the anatomy, the articles and diagrams helped me understand and remember better whereas for the treatment the podcast and interview helped me analyse and evaluate efficiently. This gives me an important lesson to not restrict my learning to any particular source or style and change it according to the need. This assignment was a good self-directed CPD course for me to improve my knowledge about shoulder instability but also aspire to soon take more CPD courses with different types of learning activities like attending workshops, shadowing, and practicing on the patients. However, the experience of writing this assignment will be a reminder of how learning might not always go according to my plans so I should always be open for to adapt to new ways of learning.
References:
Abrams, R. and Halleh Akbarnia. 2022. Shoulder Dislocations Overview. StatPearls [Internet]. Available at: https://www.ncbi.nlm.nih.gov/books/NBK459125/ [Accessed: 29 July 2023].
Advanced practice in physiotherapy Understanding the contribution of advanced practice in physiotherapy to transforming lives, maximising independence and empowering populations. Available at: https://www.appn.org.uk/cms/wp-content/uploads/2015/08/ALP-in-physiotherapy-final.pdf. [Accessed: 1 July 2023]
Baba, Y., Knipe, H., Luong D, et al. 2023. Glenohumeral ligaments. Available at: https://radiopaedia.org/articles/glenohumeral-ligaments?lang=us [Accessed: 29 July 2023].
Brukner & Khan’s Clinical Sports Medicine: Injuries, Volume 1, 5e | Clinical Sports Medicine Collection | McGraw Hill Medical. 2023. Available at: https://csm.mhmedical.com/book.aspx?bookid=1970 [Accessed: 29 July 2023].
Coulthard, C., Cairns, M., Williams, D., Hughes, B. and Jaggi, A. 2021. Management of atraumatic shoulder instability in physiotherapy (MASIP): a survey of physiotherapy practice. BMC Musculoskeletal Disorders. 22(1). https://doi.org/10.1186/s12891-021-04677-9
Dalton, S.E. and Snyder, S.J. 1989. Glenohumeral instability. Baillieres Clin Rheumatol 3(3), pp. 511–534. doi: 10.1016/s0950-3579(89)80006-8
Gibbs Reflective cycle | Crowe Associates. 2015. Available at: https://www.crowe-associates.co.uk/coaching-tools/gibbs-reflective-cycle/ [Accessed: 31 July 2023].
Gibbs’ Reflective Cycle. 2020. Available at: https://www.ed.ac.uk/reflection/reflectors-toolkit/reflecting-on-experience/gibbs-reflective-cycle [Accessed: 30 July 2023].
Goodwin, R., Moffatt, F., Hendrick, P., Stynes, S., Bishop, A. and Logan, P. 2021. Evaluation of the First Contact Physiotherapy (FCP) model of primary care: a qualitative insight. 113, pp. 209–216. doi: 10.1016/j.physio.2021.08.003
Guerrero, P., Busconi, B.D., de’Angelis, N. and Powers, G. 2009. Congenital Instability of the Shoulder Joint: Assessment and Treatment Options. J Orthop Sports Phys Ther 39(2), pp. 124–134. doi: 10.2519/jospt.2009.2860.
Investment and evolution: A five-year framework for GP contract reform to implement The NHS Long Term Plan. 2019. Available at: https://www.england.nhs.uk/wp-content/uploads/2019/01/gp-contract-2019.pdf.
Jan De Houwer, Dermot Barnes-Holmes and Moors, A. 2013. What is learning? On the nature and merits of a functional definition of learning. Available at: https://www.researchgate.net/publication/235380853_What_is_learning_On_the_nature_and_merits_of_a_functional_definition_of_learning [Accessed: 1 July 2023].
Main, P. 2022. Kolb’s Learning Cycle. Available at: https://www.structural-learning.com/post/kolbs-learning-cycle [Accessed: 31 July 2023].
Matters, P. 2015. Session 20 – Shoulder Instability - Jo Gibson & Jack Chew - The Physio Matters Podcast. YouTube. Available at: https://www.youtube.com/watch?v=N9DH_qSzA2I [Accessed: 30 July 2023].
Mcdaniel, R. 2010. Bloom’s Taxonomy. Available at: https://cft.vanderbilt.edu/guides-sub-pages/blooms-taxonomy/ [Accessed: 31 July 2023].
Miniato, M.A., Anand, P. and Varacallo, M. 2022. Anatomy, Shoulder and Upper Limb, Shoulder. StatPearls [Internet]. Available at: https://www.ncbi.nlm.nih.gov/books/NBK536933/ [Accessed: 29 July 2023].
Nicolozakes, C.P., Li, X., Uhl, T.L., Marra, G., Jain, N.B., Perreault, E.J. and Seitz, A.L. 2021. Interprofessional Inconsistencies in the Diagnosis of Shoulder Instability: Survey Results of Physicians and Rehabilitation Providers. Int J Sports Phys Ther 16(4). doi: 10.26603/001c.25170
Magee, D., Manske, R., 2021. Orthopedic Physical Assessment. 7th edition. Available at: https://www.uk.elsevierhealth.com/orthopedic-physical-assessment-9780323749510.html [Accessed: 30 July 2023].
Petty diagram • Evidence Based Teachers Network. 2017. Available at: https://ebtn.org.uk/cognitive-science/learning-cycle-s-2015-2/ [Accessed: 30 July 2023].
Physiotutors. 2023. Shoulder Instability Rehab | Early & Mid-stage | Strength & Stability. YouTube. Available at: https://www.youtube.com/watch?v=12gUmyq-6xc [Accessed: 30 July 2023].
Shoulder Instability. 2020. Available at: https://www.physio-pedia.com/Shoulder_Instability#cite_note-10 [Accessed: 29 July 2023].
Shoulder, C. 2020. Types of Shoulder Instability. YouTube. Available at: https://www.youtube.com/watch?v=GT2P0B0aoOY [Accessed: 29 July 2023].